Elevator pitch
Retirement offers the opportunity to give up potentially risky, unhealthy, and/or stressful work, which is expected to foster improvements in retirees’ health. However, retirement also bears the risk that retirees suffer from the loss of daily routines, physical and/or mental activity, a sense of identity and purpose, and social interactions, which may lead them to adopt unhealthy behaviors. Depending on the relative importance of the different mechanisms, retirement may either improve or cause a deterioration of retirees’ health, or eventually have no effect on it at all.
Key findings
Pros
Retirement is one of the most fundamental and potentially most disruptive events in an individual’s life.
Methodological innovations and access to large administrative data sets have advanced the credibility of empirical estimates.
Retirement may either be beneficial (e.g. if it is voluntary) or detrimental (e.g. if it cuts all social contacts) to retirees’ health.
The effects of retirement on health work primarily through changes in retirees’ health-related behavior.
Cons
Reverse causality makes it very difficult to establish causality.
The outcome measured and time horizon under consideration are important methodological issues.
The most credible empirical evidence available remains ambiguous.
Due to its ambiguity, it is not possible to derive uniform policy implications from the available evidence.
Individuals react differently to becoming a retiree, depending on both personal and contextual factors.
Author's main message
Knowing the health effects of retirement is important for an optimal design of pension policies. Empirical research suggests that retirement may either improve retirees’ health, reduce it, or eventually have no effects at all. This variation may best be rationalized by the existence of heterogeneous effects across groups of individuals who respond differently to becoming a retiree. This point of view not only acknowledges the startling complexity of adjustments eventually triggered by retirement, it also offers the opportunity to focus on those factors or contexts that lead to either positive or negative health effects of retirement. Importantly, it also implies that there are no uniform policy recommendations.
Motivation
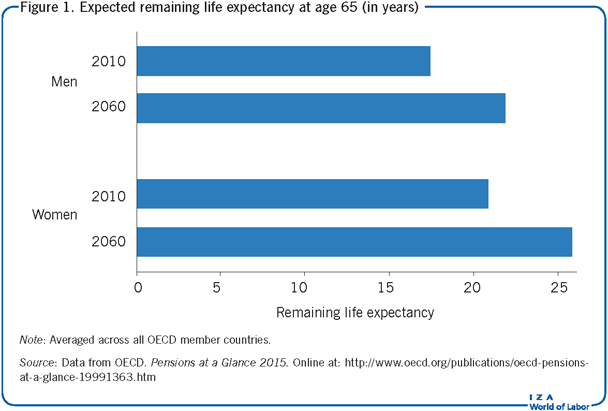
According to projections by the OECD, illustrated in Figure 1, the expected remaining life expectancy at age 65 in its member countries will further increase from 17.4 to 21.9 years for men (corresponding to a relative increase of about 26%) and from 20.8 to 25.8 years for women (a relative increase of about 24%) by the year 2060.
This increase in average life expectancy will put significant pressure on the financing of public social security systems in the years to come. In turn, this will likely necessitate pension system reforms to counterbalance the rise in aggregate pension income, including increasing the statutory retirement age and/or reducing replacement rates in the pension system.
An overall assessment of the welfare effects of such policies, however, should also take into account their potential health effects on retirees. For example, if an increase in the retirement age was associated with an improvement in retirees’ health, this would obviously make the case for such policies even stronger. On the other hand, if an increase in the retirement age would result in a deterioration of retirees’ health by, for example, triggering bad health behavior among retirees, then this might counteract the beneficial effects of an increase in the retirement age as part of the savings in spending will potentially be offset by additional health care costs.
However, the calculation of welfare effects is complicated by the fact that retirement may affect both a retiree’s health status (by influencing morbidity) as well as his/her remaining life expectancy. For example, if morbidity would increase following retirement, this would generate additional health care costs. From a welfare point of view, this would also deteriorate the quality of life of the affected individuals (i.e. by distinguishing between healthy and unhealthy years or by calculating so-called quality-adjusted life years). While such calculations are possible in practice, there are many delicate implementation and ethical issues involved. Ultimately, it is not obvious—from a policy perspective—whether one can (or should) trade off financial benefits and/or costs with longevity and morbidity.
Discussion of pros and cons
Retirement triggers a complex and multifaceted set of adjustments
The complexity of the economic and psychological adjustments initiated by retirement implies that there exist different, yet potentially interrelated, mechanisms through which retirement may affect retirees’ health. The most obvious channel is that retirees are able to leave an unhealthy, risky, and/or stressful work environment. Indeed, the idea that retirement allows individuals to retreat from stressful and/or unhealthy working conditions is often advanced as an argument against increasing the statutory retirement age; more specifically, it is often argued that workers doing heavy physical work would become especially worse off if the retirement age was increased.
That being said, it might also be the case that some people are forced to retire involuntarily (e.g. because of statutory retirement age legislation). This might have a negative effect on health, especially if forced to leave behind a job that one found interesting, meaningful, or otherwise satisfying. At the same time, retirement massively increases the time available for leisure activities. By itself, this is expected to improve retirees’ health because the “production” of health is a time-consuming activity. However, in practice, the availability of more leisure time might turn out to be a double-edged sword because leisure may also be spent in a way that is detrimental to one’s health.
Moreover, replacement rates are significantly below parity in most countries, implying that retirement is usually associated with a significant loss in disposable income. Such a reduction in disposable income is expected to have a negative effect on health because higher income is positively associated with both health care expenditure and living a healthy lifestyle. (Please note, however, that expenditure for health care is often covered by a country’s health insurance, and thus a given replacement rate may have different effects on individuals’ consumption of health care in different countries.) There might even be a lack of pension adequacy in the case of (very) low replacement rates, i.e. there might be a significant drop in consumption and/or income level and a higher risk of poverty among retirees.
Another mechanism relates to the fact that retirement disconnects people from those aspects of work that are usually thought to be important for one’s mental well-being (even if the job itself is unhealthy and/or stressful). This includes: being physically and/or cognitively active, having a daily routine, having access to a stable social network, and having a positive self-identity and a sense of meaning. Obviously, entering retirement does not necessarily imply that one loses all the “benefits” of being (self-)employed, but it is obvious that retirees have to actively arrange corresponding substitutes themselves. There is thus clearly a risk that some retirees will suffer from transitioning into retirement because they lack all or part of these beneficial aspects of work.
A final aspect that might be important relates to the degree of control the retiree has with regard to the actual timing of retirement. Specifically, everything else being equal, one would expect that retirement is less stressful if its timing is well-known in advance, such that individuals have enough time to prepare themselves for the transition from work to retirement, and if individuals are free to choose the timing of retirement themselves (as in a defined contribution system). This, however, raises the potential issue that some workers are faced with conflicting incentives. For example, retiring earlier might be good for one’s health, but early retirement might not be affordable. Finally, it is also conceivable that workers are not able to foresee how their retirement timing might affect their own health.
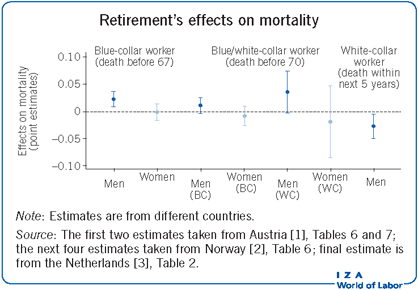
Taken together, it should be clear that the overall health effects of retirement are ambiguous from a theoretical point of view because there are good arguments in favor of there being both health improvements as well as deteriorations following retirement. In these circumstances, it is clear that empirical estimates are necessary to inform whether the positive or the negative effects dominate; however, it is important to be aware that empirical estimates may yield different estimates depending on the specific context of the study (i.e. depending on the context, either effect could ultimately dominate). This is also evident from the Illustration, which shows estimated effects of retirement on mortality in different contexts (i.e. the studies use data from different countries and use different methods).
Methodological issues
There are a couple of methodological issues that make the estimation of the causal health effects of retirement quite a demanding task.
Reverse causality
The most important methodological issue in determining the health effects of retirement is due to the possibility that causality does not only run from retirement to health, but also the other way around. Indeed, in the context of retirement, there is most likely selection into early (or earlier) retirement based on ill health (i.e. individuals in bad health are more likely to retire early/earlier than those in good health). In this scenario, simply ignoring, or not properly dealing with, the issue of self-selection into (early) retirement will tend to produce estimates of the health effects of retirement that have no causal interpretation and that are too negative. In fact, many of the more recent empirical studies support the claim that there is negative (in terms of health) selection into early or earlier retirement. These studies can empirically support the claim because they report both estimates that do and that do not take the issue of reverse causality into account.
While earlier studies tended to neglect the issue of reverse causality, more recent studies usually try to carefully address this issue using different methodological tools, most notably instrumental variable methods (e.g. [1], [2], [3]) or regression discontinuity design (e.g. [4], [5]). One important downside of these approaches, however, is that they usually yield estimates of the health effects of retirement that are tied to (often very) specific subpopulations because the underlying policy changes, on which the empirical designs were essentially built, target such specific groups. For example, one study uses a targeted retirement offer made to military officers aged 55 or over in Sweden to estimate the health effects of retirement [6]. While looking at this policy is useful for estimations of the subpopulation actually affected by it, there is reason to expect that the estimated effects do not easily extend to the more general population.
Country-specific institutional rules
Many of the available empirical estimates are also, though only implicitly, influenced by institutional arrangements that are specific to a given country, and often also specific to different parts of the working population. Most importantly, perhaps, countries differ both with respect to the statutory retirement age and the effective replacement rate. It is therefore conceivable that estimates from different countries yield different estimates of the health effects of retirement because they focus on different aged workers who may, for that reason, react differently to the transition into retirement. Differences in the replacement rate imply that the loss in disposable income differs across countries and should be factored in when comparing estimates internationally. Another difference between countries, already mentioned above, is the financing of health care expenditure.
Choice of health outcomes and time horizon under consideration
Another potentially relevant methodological aspect is the choice (or simply the availability) of different outcome variables used to pin down the health effects of retirement. The most important distinction in this context is the one between subjective (such as self-evaluations of one’s physical or psychological health) and objective measures of health (such as indicators of premature mortality or of the presence of specific diseases). Because health is such a complex and multifaceted phenomenon, subjective health measures are clearly helpful in many research contexts, at least as a complement to objective health measures. However, the main concern in the context of the effects of retirement on health is that the decision to retire early might also influence the reporting of subjective health measures because, for example, people tend to vindicate their own choices. For instance, one study finds positive effects of retirement on subjective but not on objective health measures, using the identical data set and the same empirical strategy—suggesting that one needs to be somewhat cautious when using subjective measures in evaluating the health effects of retirement [7].
Among the large set of potentially available objective health indicators, mortality, ideally enriched with information about the cause(s) of death, is presumably the preferred one among economists because it is the most objective and the most encompassing measure available. In the context of retirement, there are many potential channels—that are eventually correlated with each other—through which health might be affected, and thus broader health measures (e.g. mortality) should be favored over more specific measures, whenever available.
A final issue worth pointing out is that the short-term effects of retirement may be different from its longer-term effects because changes in health behavior—representing the most important causal mechanism—most likely do not have immediate, but only delayed effects [8], [9]. For example, if retirement triggers bad health behavior such as more intense smoking and drinking or less exercising, then this change in behavior will only show up some considerable time after retirement.
Diverse and ambiguous estimates of the causal effects
There has been quite a surge in the number of empirical studies trying to estimate the causal effects of retirement on health in the past couple of years. Given the importance of the methodological issues mentioned in the preceding section, the following discussion focusses on those studies that use an empirical setup that is in principle able to deal with the issue of reverse causality.
Studies that focus on mortality as an outcome measure
One of the first empirical studies using a credible research design to estimate the causal effect of retirement on mortality uses a unique change in Austria’s unemployment insurance to identify the causal effect of early retirement on mortality [1]. This change ultimately allowed some workers to retire up to 3.5 years earlier than comparable workers. The study finds that retirement causes an increase in the probability of dying before the age of 67 among blue-collar men (birth cohorts 1929–1941), but not among blue-collar women (born 1934–1941). A unique feature of this study is that the underlying policy change arguably pushed many workers involuntarily into early retirement. For the US, and exploiting the fact that there exist age-based discontinuities in the eligibility for social security, it is found that male mortality (at age 62) increases due to retirement [5]. The sample also includes women, but the effect on women is not significant. A further study using administrative data from Norway relies on a program that reduced the eligibility age for early retirement to estimate the effect on mortality for both blue- and white-collar workers (born between 1928 and 1938) [2]. It finds that early retirement does not affect mortality (i.e. death before the age of 70), at least when selection into retirement based on health is taken into account. For the Netherlands [3], as well as for Sweden [6], targeted early retirement offers have been used to estimate the effect of retirement on mortality. Both studies focus on specific subpopulations because the retirement offers were not available to the general population (only civil servants in [3], and male military officers in [6]). Both studies conclude that retirement has a beneficial effect on the risk of death. A 2013 study is the only one that looks at a policy change that actually increased the incentives to retire later (instead of reducing them), using survey data from France covering only private sector employees [10]. It also finds that retirement increases the risk of mortality. Thus, taken together, the different studies report heterogeneous estimates, varying from negative to null to positive health effects of retirement on mortality.
Other objective health measures
Considering such variation in findings, it is perhaps not too surprising that studies using alternative health outcomes yield diverse results concerning the effects of retirement as well. For example, while one study reports estimates that suggest that retirement has a detrimental effect on various objective measures of health [11], such as indicators of whether an individual has experienced a chronic disease (for instance, diabetes or a heart attack), several other studies using objective health measures other than mortality report positive effects of retirement on health [4], [12]. Similarly, studies that focus directly on the effect of retirement on individuals’ health behavior (such as smoking, drinking, and choice of diet) also yield inconsistent results.
Subjective health measures
For subjective health outcomes the estimates appear somewhat less ambiguous, as the majority of the empirical studies on these measures report positive effects of retirement (e.g. [4], [7], [13]), though there are the usual exceptions to the rule (e.g. [9]). As discussed above, however, subjective health measures might be biased toward finding (too) positive estimates of the health effects of retirement.
Under what circumstances does retirement (not) trigger ill health?
The observable variation in the estimated health effects of retirement primarily relates to the fact that most studies focus on specific groups of individuals that were usually subject to specific interventions in specific institutional contexts, rather than to methodological issues (even though some issues remain with the most recent studies). Thus, presumably, the estimates from most of these studies do not directly apply to alternative contexts.
At the same time, however, the available empirical evidence might offer some hints concerning factors that potentially mediate the effect of retirement on health. A first factor is individuals’ identification with their previously held job (or with work in general). Moreover, it is quite obvious that the health effects depend on the type of job/work done before entering retirement. Another aspect that could be important in this regard is the voluntariness of the retirement decision. Indeed, it seems again quite obvious that an involuntary retirement has different effects on retirees’ health than a voluntary decision to retire ([1] provides some indirect evidence on this, finding that it is mainly men entering early retirement involuntarily who experience negative health effects). Relatedly, it may also be relevant whether (or not) the timing of retirement can be anticipated (well) in advance, and whether there is a strong norm toward work in general and/or toward retiring at the regular age. Retirement that is anticipated well in advance (even if involuntary) is presumably less stressful, as is retirement in an environment characterized by a weak norm toward work in general.
To complicate things even further, it is also conceivable that these factors only take full effect if individuals are predisposed in some way toward showing negative health effects upon retirement. For example, being (involuntarily) pushed into retirement may only be detrimental to one’s health if there already exists, say, a predisposition toward ill health behavior (e.g. heavy smoking and/or few or no physical activity outside the realm of work).
Limitations and gaps
The empirical literature on the health effects of retirement has made significant advances in the past few years, due to both methodological innovations as well as to (easier) access to large administrative data sets that often cover detailed and objective information on individuals’ health status. Thus, the more recent empirical evidence on the health effects of retirement has clearly become much more credible than earlier studies on the same subject. Nonetheless, there remain a couple of limitations and gaps.
A first limitation is that there are still some methodological caveats to several of the studies discussed above. For example, many of them use policy discontinuities in age to estimate the health effects of retirement. While these discontinuities are usually set arbitrarily (from the retirees’ point of view), which makes them a priori suitable from a methodological point of view, it is nonetheless the case that individuals usually have considerable leeway over the effective timing of their entry into retirement (i.e. such policies may change the earliest age at which workers can retire, but not necessarily the effective retirement age because an individual may still decide to retire later). This limits the analytical value of the policies’ arbitrary age cutoffs.
A more subtle issue is that the empirical evidence regarding the health effects of retirement rests exclusively on estimates of policy experiments that allowed for earlier (than regular) retirement. In this regard, it is important to keep in mind that there does not necessarily exist a symmetry in the effects on health from preponing and postponing the retirement age. That is, even the best estimates available might not be informative about the effects of policies that increase the regular retirement age (the kind of policies most likely implemented in the future).
A further issue that needs clarification is how the estimates on the health effects of retirement square with the (empirically well-established) finding that involuntary job loss leads to a deterioration in health and even an increase in mortality. This contrasts strongly with the huge variation in estimates (particularly positive ones) of the causal health effects of retirement.
A final gap in the literature is that most studies (still) try to estimate “the” causal health effect of retirement, in the hope that their estimates will generalize to very different contexts. However, given the theoretical ambiguities as well as the specificities of retirement regulations at the country level, it appears much more reasonable to accept that the quest for uniform health effects of retirement is most likely elusive. A more modest, but also more realistic, perspective acknowledges that retirement can have either (as well as both) positive or negative effects on retirees’ health. Such a perspective would also help to shift the focus toward finding those factors that determine whether retirement ultimately leads to an improvement or an impoverishment of health. A systematic review of the available empirical literature and a meta-analysis on the basis of such a review have the potential to yield significant insight into the factors that trigger either negative or positive health effects of retirement.
Summary and policy advice
Understanding the health effects of retirement is important for conducting an overall assessment of policies that aim at changing key parameters of the retirement system; however, several distinct methodological issues make it very difficult to precisely pinpoint these effects in practice. In addition, there are good theoretical reasons to expect that the health effects of retirement are not uniform but rather heterogeneous across different contexts and/or different subpopulations of workers.
For these reasons, it is not surprising that the available empirical evidence on the causal health effects of retirement remains somewhat inconclusive. While some studies find that retirees suffer from health deterioration, others report that the health status among retirees improves. While even those studies that apply the best available research designs suffer from methodological issues, it is perhaps more likely that a significant part of the observed heterogeneity in the available estimates is simply due to the fact that most studies identify effects that are tied to specific institutional contexts and/or subpopulations of retirees. This suggests that there is considerable variation in the health effects of retirement across different contexts and/or subpopulations.
Unfortunately, this heterogeneity in the empirical estimates makes it difficult, or even impossible, to derive any firm and uniform policy conclusions. Nonetheless, the available evidence does suggest a couple of tentative policy recommendations. First, it appears that some groups of workers (e.g. men compared to women) are more prone to, and that some institutional factors (e.g. being involuntarily pushed into retirement) promote, unhealthy behavior after retirement. This begs the question of whether it would make sense to apply different retirement ages to different parts of the working population. Second, given that retirees’ health behavior is the primary causal mechanism, it might be worthwhile to think about instruments to encourage good health behavior among retirees (e.g. by providing subsidies for services promoting good health).
Acknowledgments
The author thanks an anonymous referee and the IZA World of Labor editors for many helpful suggestions on earlier drafts. Previous work of the author contains a larger number of background references for the material presented here [1].
Competing interests
The IZA World of Labor project is committed to the IZA Guiding Principles of Research Integrity. The author declares to have observed these principles.
© Andreas Kuhn