Elevator pitch
Research has shown that job insecurity affects both mental and physical health, though the effects are lower when employees are easily re-employable. The detrimental effects of job insecurity can also be partly mitigated by employers allowing greater employee participation in workplace decision-making in order to ensure fair procedures. But as job insecurity is felt by many more people than just the unemployed, the negative health effects during recessions are multiplied and extend through the majority of the population. This reinforces the need for more effective, stabilising macroeconomic policies.
Key findings
Pros
Many cross-sectional studies in epidemiology, psychology, and economics show a strong connection between job insecurity and poor physical or mental health.
Some longitudinal studies show that the effects of job insecurity on health are causal, particularly in relation to mental health, headaches, eyestrains, and skin problems.
The size of the effect of job insecurity on health can be as large as the effect of unemployment.
Cons
Many cross-sectional and longitudinal studies do not prove causation, and there are a few countries in which no association is found.
Longitudinal studies confirm that the harmful effects of job insecurity on health are mitigated when employees are re-employable.
Employee participation and social support are associated with higher well-being, and may help in situations of high insecurity.
Little is known about how people may or may not adapt to job insecurity over time or how they may compensate for the associated uncertainty.
Author's main message
Job insecurity has become an increasing problem since the great recession and as labor markets have become more flexible. It is well established that job insecurity, like unemployment, has causal detrimental effects on mental and physical health. Workers’ health is not just a matter for employees and employers, but also for public policy. Governments should count the health cost of restrictive policies that generate unemployment and insecurity, while promoting employability through skills training. Policy should also encourage forms of employee participation and social support in workplaces.
Motivation
In the years between 2000 and 2013 the average unemployment rate in OECD countries rose from 6.0% to 7.9% of the labor force, with considerable variation between countries. The overall rise might not sound like much, but the impact of increased unemployment extends far beyond just those who are unemployed and their families. When unemployment rises, those who remain in work tend to experience an increase in job insecurity. Major recessions, such as the one that followed the financial crisis of 2008, are therefore far-reaching in their effects across society. There is as a result considerable interest in understanding whether, and to what extent, job insecurity is a significant cause of poor physical or mental health. Such health costs should be a potential concern for macroeconomic policymakers who control economic stability, and for health and employment policymakers and other social partners who might be able to ameliorate the deleterious effects of insecurity.
The phrase “job insecurity” refers mainly to the fear of losing one’s job. For some, however, the expression is broader and refers to the possibility of some sort of degradation of status in a job without actually being made redundant, such as being transferred to a less interesting or less challenging post with the same employer. Such “job status” insecurity has been increasing in the UK since at least 2000, but there is little scientific evidence about its effects on health and well-being. This contribution therefore focuses entirely on the form of job insecurity that is related to the fear of losing one’s job.
Understanding the effect of job insecurity is not a simple matter, as high perceptions of insecurity may be held by workers who already have particular health characteristics, or who are undertaking jobs in which there are other detrimental aspects in terms of job quality. Only some of these other factors can be easily observed and controlled for in a scientific study.
The consequences of insecurity may also depend on factors that moderate the detrimental effects—at both organizational and societal levels. If employers and policymakers are to better understand and ameliorate the effects of insecurity in organizations and in society, some knowledge of the practical significance of these moderating factors is needed.
Discussion of pros and cons
A British politician once dismissed fears of unemployment as being “all in the mind,” because this insecurity existed at a time of growing employment. However, even in good economic times there are some who fear job loss. Moreover, while there is some tendency for overall pessimism, it has been shown that those people who report a high probability of job loss in the coming year are much more likely than others to actually lose their jobs in that time [1]. In the aggregate, insecurity tends to be higher in countries with high unemployment, and to increase in each country when unemployment increases, exactly as one would expect [2].
Job insecurity and choice
In an uncertain world there are few jobs that do not carry with them some degree of insecurity. Indeed, insecurity can be thought of as a disamenity, or an unpleasant disadvantage of a job, in much the same way as it would be to have to accept working in harsh physical conditions. If workers could choose the level of insecurity they are prepared to accept, those who greatly dislike risk would shun insecure jobs, while risk-lovers would opt for the insecure jobs. With the risk-averse in the large majority, insecure jobs would acquire a premium that compensates for the disamenity of the insecurity. Although the insecurity may pose a health risk for the risk-lovers in the insecure jobs, their higher pay could compensate for this. As an illustration, few people would suggest that the insecurity faced by modern football managers should be a matter for public policy measures, given their relatively very high salary levels.
While trade-offs between pay and risk are widespread, the choice typically facing those in insecure jobs is not between more-secure or less-secure jobs, but between insecure or no jobs. Constraints on choice arise because people’s circumstances change, for example through their employers’ fortunes, or more generally through varying macroeconomic circumstances. The phenomenon of employees finding themselves in jobs with far less security than they would choose can become especially widespread in times of recession.
It is mainly the workers themselves whose mental and/or physical health may be affected when their insecurity is raised. But the effects of insecurity go beyond the individual. Similarly, and of particular interest, are the “survivors” of company downsizing. If the health and, consequentially, the effectiveness of these workers are impaired, it is not only them but their organizations that suffer. In addition, the families of insecure workers experience the effects of potential income loss and stress, and so do societies more broadly, in that they must provide care through health systems. Job insecurity is therefore a wider issue than simply a matter for individual choice.
How job insecurity can affect mental and physical health
Whether or not employees’ fears of losing their jobs are justified, their feeling of job insecurity may nevertheless have detrimental effects on their health, for a number of reasons. The economic reason is that a high probability of job loss indicates a likely period of unemployment and lower income in the future. A person’s expected long-term income, averaged out over a period of years, is thus lowered as a result of the insecurity. In addition, those with few savings to fall back on may be seriously compromised by the loss of income following job loss. Since income is related to health, one could therefore expect the loss of expected income that derives from insecurity to lead to impaired health.
However, economic deterioration may be less important than the psychological loss of identity and meaning attached to jobs. Studies of unemployment have found that its impact on health is much greater than can be explained simply by the loss of income resulting from unemployment. An important psychological aspect of job insecurity is the stress associated with the uncertainty. Psychological studies of job insecurity have emphasized how job insecurity should be categorized as a significant cause of stress.
While low levels of stress may be beneficial, in terms of motivating people to work harder, there is abundant evidence for the detrimental effects on physical and mental health of high or prolonged stress. In addition, other side effects have been hypothesized: for example, that high levels of job insecurity prompt low motivation and compliance with safety efforts, hence higher workplace injuries.
Empirical evidence linking insecurity to types of ill-health
There is a considerable amount of evidence to show that, on average, employees in jobs perceived to be insecure tend to have worse health. One recent study combined several smaller studies (using a meta-analysis) from Denmark, Finland, the US, Sweden, Germany, the UK, and Belgium [3]. The study found a link between the perception of job insecurity and the subsequent experience of coronary heart disease: on average, those with high job insecurity have a 32% greater risk of heart disease than those in highly secure jobs. However, the authors also found that the people who were more insecure were, in any case, disproportionately drawn from groups with a high risk of heart disease. For example, people with high job insecurity were found to take less physical exercise and to have a higher prevalence of hypertension. Once these and other confounding factors were taken into account, the average elevated risk was reduced to 19%. Because insecurity is often measured rather imprecisely, this association may be an underestimate. However, the constituent studies are all cross-sections, and it is not claimed that this estimate shows a causal impact of insecurity on heart disease.
In another recent study it has been shown that across 16 European countries there is a robust statistical association between insecurity and poor health among older employees [4]. The study finds that employees who reported that their “job security was poor” were 39% less likely to report that their health was good or very good (as opposed to fair, poor, or very poor). Looking at how the effects vary across individual countries, the study finds significant detrimental effects of insecurity on health in the Czech Republic, Denmark, Germany, Greece, Hungary, Israel, the Netherlands, Poland, and Russia. In two countries, Belgium and Sweden, no effect was found.
Despite the wide scope of this study and its application to quite large representative samples in each country, in keeping with other cross-sectional studies it did not claim that the association was causal. The problem is that the insecurity may be “endogenous,” i.e., affected by some other relevant factor(s), so that associations cannot be interpreted as causal. It might be the case that for some reason it is the less healthy individuals who are channeled into the less secure jobs (“reverse causality”). Hence, there is an association between health and insecurity but the direction of causality is not clear cut. Or it could be that there is some unknown factor surrounding workplaces and employees that simultaneously makes them both less healthy and less secure.
Nevertheless, the breadth and strength of such cross-sectional findings should not be ignored. Many other cross-sectional studies, with varying indicators of poor health or low well-being, present the same picture, often taking into account several confounding factors.
In the relatively few studies in which researchers have been able to investigate causal effects more effectively, the results of the cross-sectional studies are not always found to be robust, though sometimes they are.
A striking recent study finds one way around the problem of insecurity being endogenous [5]. In a multi-country European study the researchers found that job insecurity was associated with some specified ill-health conditions—namely backache, muscular pain, headaches or eyestrain, stomach ache, depression or anxiety, overall fatigue, and insomnia. However, they were rightly concerned that these cross-sectional associations might not be due to a causal process. To address this, they took advantage of the fact that countries have different laws about employment protection. The authors argued that perceptions of job insecurity would increase in countries or regions where employment protection was at a low level, and that this would especially matter in industries known (from external evidence) to have high dismissal rates. Their study examined the effects on health of the insecurity that arises from low employment protection. Their approach depended on the assumption that individual employees would not be able to alter the regulations pertaining to them.
Remarkably, the study finds that job insecurity has substantial causal effects on headaches, eyestrains, and skin problems. Moreover, it did not find that, for these outcomes, the cross-sectional associations were underestimating the causal effects. It also finds that job insecurity stimulates a low level of overall (self-reported) health, though the authors could be less confident of this finding because it carried an especially wide margin for error, including the possibility of a zero effect.
Finally, by contrast, the authors found that job insecurity, when stimulated by low employment protection, was not the cause of the other possible outcomes (including cardiovascular disease, depression, muscular pain, and insomnia) with which it was associated in the cross-section. Of course, job insecurity can arise for reasons other than low employment protection, so the authors caution that their study does not rule out the potential impacts of job insecurity on these other health outcomes.
The value of longitudinal studies in determining causality
Another way of partially accounting for hidden factors that make job insecurity endogenous is by using longitudinal data, i.e., data gathered over long time periods, which look at how the health of a particular group of individuals changes when their job insecurity changes. This method sidesteps those hidden characteristics of individuals that do not change over time, such as personality traits that lead them to give unduly optimistic or pessimistic reports about their health and working conditions.
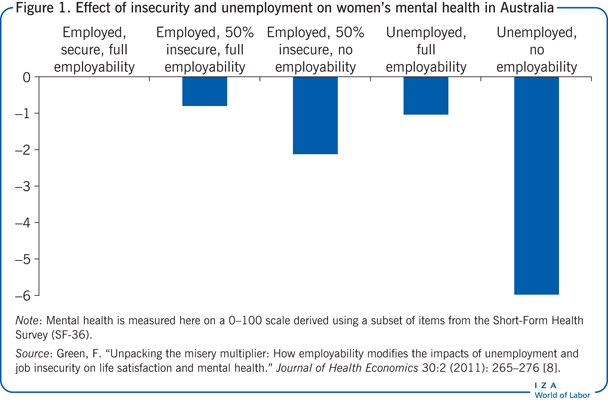
One longitudinal study examined the effect of job transitions on mental health in four countries: Australia, Canada, Switzerland, and the UK [6]. In every country it was found that moving from a secure to an insecure job resulted in a substantial increase in mental distress. This was the case whether the job was a standard one (full-time and with a permanent contract) or a non-standard one. Similarly, when individuals moved from a state of non-employment into employment, the effects on their mental health depended greatly on whether the new job was perceived to be secure. Where the job was thought to be very secure, it led to a significant reduction in mental distress. At the opposite extreme, if the new job was perceived to be very insecure, its positive effects on mental health were much reduced or even zero. In the case of unemployed men in Australia, the new job that was very insecure even increased mental distress—in other words, Australian men were better off, from the perspective of their mental health, not being employed than being employed in a very insecure job.
To a considerable extent, the perception of insecurity is associated with the type of contract, with those on temporary contracts inevitably feeling more insecure. Moving from non-employment into a job with a temporary contract was beneficial for mental health in Australia and the UK, but not at all beneficial in Switzerland.
In another longitudinal study from Italy, there is further evidence that temporary contracts are a source of ill-health [7]. Nevertheless, the association between contract status and security differs across countries, depending on employment regulations and whether temporary contracts are regularly renewed. Temporary jobs may also differ in other ways from jobs with permanent contracts, usually for the worse—for example, they tend to have lower degrees of autonomy. Thus, unless one can take into account these other facets of job quality, the relationship between temporary contracts per se and health cannot be considered as decisive evidence for the effect of insecurity on mental health.
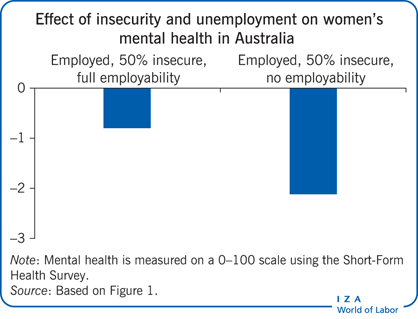
A further, large-scale longitudinal study examines the effects of job insecurity on mental health and life satisfaction in Australia [8]. The indicator of insecurity used in this study is the probability of job loss as estimated by workers themselves, which is a measure other studies have validated. The advantage of this measure is that we can be confident that we are not mixing up the probability of job loss with any wider sense of insecurity concerning one’s status at work. The study finds that an increase in the probability of job loss stimulates a notable fall in both the mental health scale and in life satisfaction. Mental health, in this study, is measured on a 0−100 scale derived using a subset of items from the Short-Form Health Survey (SF-36). Those responding low values on this scale are more likely to be experiencing depression. The Illustration and Figure 1 show the values on this scale of various states, relative to being in a secure job and being fully employable. Accordingly, the loss of mental health from being partially insecure (i.e., having a 50% chance of job loss within a year), while remaining fully employable (i.e., being sure of getting an equally good job), was close to the loss incurred through actually being unemployed. The effect is around an eighth of a standard deviation of the mental health scale, indicating a significant effect on the numbers suffering mental depression.
A similar effect of insecurity is found for German workers, again using longitudinal data [9]. This study discovered that the health-reducing effects of job insecurity could still be seen when the job insecurity was induced by company downsizing. This finding suggests that it is less likely that we are seeing the effects of reverse causation from personal ill-health to job insecurity.
While studies using longitudinal data are generally the most convincing ones for understanding causal processes, studies of successive cross-sections are also useful if one is aiming to understand changes in the health and well-being of a population over time. Such studies are rare owing to data shortages, but have come more into the spotlight following the great recession in 2008, with consequent concerns that job loss would be accompanied by deteriorating health. Indeed, one study has shown that job-related well-being fell in the UK either side of the great recession (between 2006 and 2012), and that this is attributable, in part, directly to rising job insecurity, an increase in the pace of workplace change, and to changing work effort and workplace participation [10].
How the effects of insecurity might be reduced or counterbalanced
Given the evidence that job insecurity has substantive effects on health, it is clear that policymakers could make a contribution to the health of populations by limiting the extent of job insecurity through proactive macroeconomic stabilization policies. Accepting, however, the fact of macroeconomic failures (such as those evidenced in the recent great recession) and that even with good macroeconomic policies there will always be a base level of unemployment and insecurity, what can health policymakers, employment policymakers, or other social partners do to ameliorate the health effects of insecurity?
The support of the health services, including awareness of job-security-induced stress and ill-health, and strategies for dealing with these, should be an evident concern of health ministers. In addition, however, there are policies and approaches that other actors can consider. Three broad areas are promising.
First, it has been shown that re-employability can go a long way toward mitigating the effects of insecurity. While the prospect of a new equally good job might not be quite as desirable as keeping one’s current job, it can prevent the loss of income and go a long way to ameliorating the psychological loss. A study using Australian data has shown, for example, that the mental health cost of job insecurity for a woman who is sure of finding a new equally good job is lower by as much as two-thirds, compared with a woman who has no hope of finding a new job (see the Illustration, comparing the first two bars) [8]. In Germany it is found that, while low job security has substantial negative effects on mental health, this is especially exacerbated in the case of women who have low re-employability. Thus, macroeconomic and microeconomic policies to stimulate individuals’ chances of re-employment would be beneficial. Welfare policies that reduce the income loss from unemployment also reduce the economic risks. Combined with active labor market policies and skills policies that enhance employability this ensemble has been termed “flexicurity” policy.
Second, the ill-health effects of negative shocks and job insecurity can be counterbalanced within organizations by forms of participation that allow both full communication with affected workers and some influence over decision-making. Participation facilitates the sense of fairness and procedural justice, and has been shown to be related to well-being, especially where companies are downsizing. Nevertheless, no amount of participation can remove the distress of job loss.
Third, social support, either from within the workplace or from outside, has a beneficial impact on well-being and workers’ mental health. Moreover, it can be of particular importance at times of insecurity. Support can be psychological, thus diminishing the threats to workers’ sense of identity when faced with insecurity; it might also be economic or industrial relations support. Studies have identified both unions and families as potential sources of social support at times of insecurity.
Limitations and gaps
A limitation to our knowledge of the health effects of job security is the insufficient breadth of coverage of longitudinal studies. It is likely that the stress effects of insecurity are the source of mental health distress, including depression, but the latter is often also associated with physical health consequences. We are not yet able to specify with confidence which forms of physical health risk are attributable to job insecurity. Nor have researchers analyzed in detail how the health effects of insecurity might extend to households.
Especially important for policy purposes, we still lack good evidence for the potential role of different forms of employee participation and of social support. While their effects on well-being have been studied, it is not known how effective they are in specifically lessening the negative effects of insecurity.
Longitudinal studies could also be used to examine the dynamics of insecurity and health. While several smaller-scale longitudinal studies, focusing on particular occupations or groups of workers, paint the same picture as the large-scale studies described above, we know little about how people may or may not adapt to insecurity over time. Are the ill-effects of job insecurity chronic, in the sense that they build up over time, as with the effects of a prolonged state of stress? Or are they more of a shock effect, immediately apparent for a year or two, but something that people get used to after a while? Do people find ways for compensating for the uncertainty?
It is very welcome to see that the study of insecurity is a lively area of scientific investigation in at least three fields—i.e., epidemiology, psychology, and economics. Yet there needs to be more communication between these fields: policymakers are not served well by discipline-based researchers who do not acknowledge valuable contributions on the same issue by those situated in other domains.
Summary and policy advice
We know from an abundance of research studies that people whose jobs are less secure experience worse health, and in a number of ways—both physical and mental—than those in secure jobs.
A small number of large-scale studies using representative data from across countries, and some smaller-scale longitudinal studies, have confirmed that some aspects of the insecurity−health association are indeed causal. In other words, when circumstances lead jobs to become insecure, employees’ health is impaired in some dimensions.
Research also shows that re-employability—i.e., the probability of being able to find another equally good job in the event of job loss—makes a substantial difference and mitigates some of the negative effects of job insecurity.
Furthermore, there is reason to expect that by facilitating participation to enable fair procedures in organizations, and facilitating social support for employees wherever possible, the detrimental effects of insecurity on health may be partly mitigated and partly countered by opposing factors beneficial for health. The evidence in this area of knowledge, however, is thin and most in need of further investigation.
Job insecurity can become especially widespread in times of recession. Although the effects are initially felt by the workers, the health consequences of each individual also extend to organizations, workers’ families and, hence, to societies which must provide care through health systems.
Workers’ health is therefore not just a private matter for employees and employers, but also a matter for public policy. Governments should take into consideration the health cost of restrictive policies that generate unemployment and insecurity, while promoting employability through, for example, skills training. Policy should also encourage forms of employee participation and social support in workplaces to mitigate the negative health effects arising from insecurity.
Acknowledgments
The author thanks an anonymous referee and the IZA World of Labor editors for helpful suggestions on an earlier draft. Previous work of the author contains a larger number of background references for the material presented here and has been used intensively in all major parts of this article [8], [10]. The figures in this paper use unit record data from the Household, Income, and Labour Dynamics in Australia (HILDA) Survey. The HILDA project was initiated and is funded by the Australian Government Department of Families, Housing, Community Services and Indigenous Affairs and is managed by the Melbourne Institute of Applied Economic and Social Research. For his research on job quality, including insecurity, the author received financial support from the Economic and Social Research Council and from the UK Commission for Employment and Skills.
Competing interests
The IZA World of Labor project is committed to the IZA Guiding Principles of Research Integrity. The author declares to have observed these principles.
© Francis Green