Elevator pitch
Childhood obesity has been rising steadily in most parts of the world. Popular speculation attributes some of that increase to rising maternal employment. Employed mothers spend less time at home and thus less time with their children, whose diets and physical activity may suffer. Also, children of working mothers may spend more time in the care of others, whose childcare quality may vary substantially. While a majority of US studies support this hypothesis and have clear policy implications, recent studies in other countries are less conclusive, largely because institutional arrangements differ but also because methodologies do.
Key findings
Pros
The association between maternal employment and childhood obesity varies regionally, with inconsistent findings.
There is little evidence that working mothers spend less time with their children.
Maternal employment might reduce obesity through healthier lifestyles, including higher quality diets and more physical activity.
High-quality childcare has a positive effect on child development and may influence childhood obesity.
By helping a family escape poverty, maternal employment could improve children’s weight outcomes.
Cons
The rise in maternal employment is related to the rise in childhood obesity.
Having a mother working non-standard or long hours is associated with childhood obesity.
Maternal employment might reduce time spent with children, which could in turn increase childhood obesity.
Maternal employment might lead to unhealthier diets and sedentary behavior among children, thereby increasing childhood obesity.
Maternal employment could increase childhood obesity if external care is of lower quality.
Author's main message
Much of the research finds that maternal employment increases the likelihood of children being overweight or obese. This association is driven by worse diets, increased sedentary behavior, and lower quality sleep for children whose mothers work. However, because a majority of mothers in developed countries want or need to work, the question cannot be whether they should stop working but whether sufficient formal and informal high-quality childcare is available and affordable. Policy measures should aim to provide parents with greater flexibility to spend time with their children and should support high-quality, affordable childcare.
Motivation
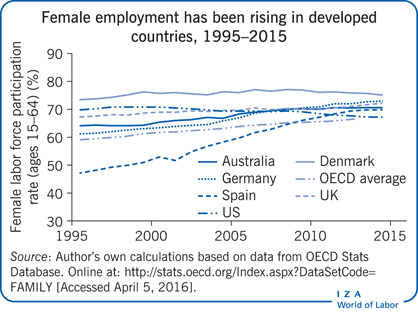
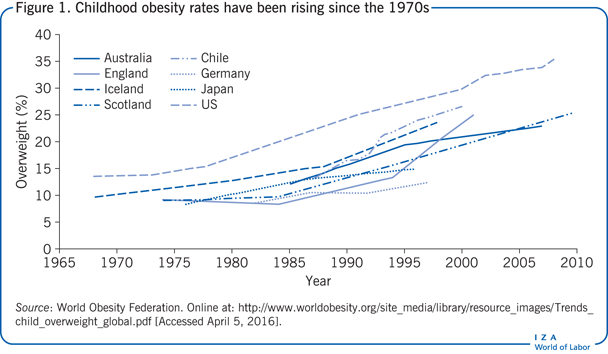
Childhood overweight and obesity rates have doubled worldwide since the 1970s, resulting in about 200 million overweight and obese children in 2014. Some 22% of girls and 24% of boys are overweight or obese. Although prevalence seems to have flattened or even decreased in some countries (Australia, France, and Sweden, for example) over the last decade, it is still high. This high prevalence is concerning because of obesity’s harmful effects on children’s emotional and physical health and the high likelihood that childhood obesity will transmit into adulthood. Childhood obesity is associated with elevated risk of cardiovascular disease, diabetes, and lowered life expectancy even when formerly obese children lose excess weight in adulthood. Because the probability of receiving medical care is significantly higher for obese and overweight children than for normal-weight children, health care costs are much higher too. Any potential explanation for the childhood obesity epidemic must also involve the parental environment. One noteworthy change over this time that has influenced family life is the increase in female employment. In OECD countries, the female labor force participation rate rose steadily from 59% in 1995 to 67.2% in 2014 (see Illustration).
Discussion of pros and cons
The association between maternal employment and childhood obesity
Over the last four decades, many developed countries experienced a simultaneous increase in childhood obesity (Figure 1) and female employment. But while the rise in childhood obesity coincides with the rise in maternal (female) employment, there are some inconsistencies in the empirical evidence.
The relation between maternal employment and childhood obesity varies across regions, cultures, and societies. For example, US studies, which dominate the research, offer strong evidence that maternal employment affects childhood obesity. This finding is supported by studies for Canada, Germany, Japan, Spain, and the UK. However, studies for Australia, China, Denmark, and Europe find little evidence that maternal employment is a risk factor for being overweight or obese in childhood. The European study investigates the correlation between maternal employment and childhood obesity for children aged 2–9 in 16 regions in eight European countries (Belgium, Cyprus, Estonia, Germany, Hungary, Italy, Spain, and Sweden) and finds little evidence of an association [1]. The same is true for the Chinese study, which uses data from five waves of the China Health and Nutrition Survey and finds no correlation with maternal employment among children ages 3–17 [2]. The Australian study, which looks at children aged 5–15 using data from the representative South Australian Monitoring and Surveillance System, finds no correlation between maternal employment and childhood obesity either [3]. The Danish study of children 7.5 years old using data from the Danish Longitudinal Survey of Children even finds a beneficial correlation between maternal employment and childhood obesity [4].
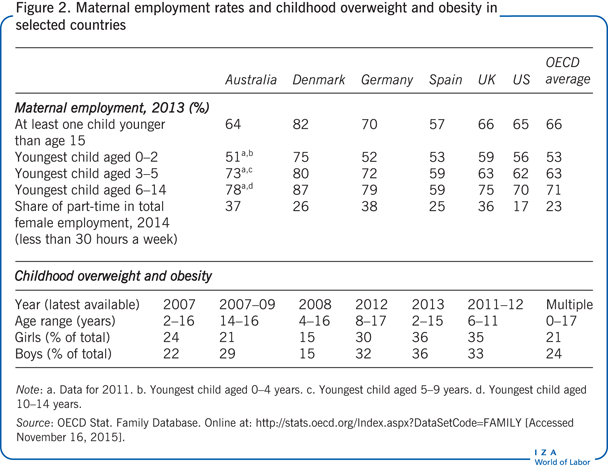
One reason for the regional differences could be variations in the labor market. Denmark, for example, has the highest maternal labor market participation rates among OECD countries, at 75% for mothers with a child aged 2 or younger and 80% for mothers with a child aged 3–5 (Figure 2). For the other countries shown in Figure 2—Australia, Germany, Spain, the UK, and the US—the share of working mothers is much lower. On average in OECD countries, 66% of mothers are employed. Maternal employment rates are below average in countries like Spain (57%) but far above average in Scandinavian countries like Denmark (82%). Working parents, especially mothers, also favor part-time employment, which accounts for 23% of all employed women across OECD countries. Australia, Germany, and the UK also have high part-time rates among women, with work hours rising as children grow older. However, part-time work is less common in Denmark, Spain, and the US relative to the other countries shown.
The institutional setting related to maternal employment
The association between maternal employment and childhood obesity is to a large extent driven by the institutional setting and the corresponding policy measures that influence maternal employment. In particular, public policies related to childcare and parental leave (Figure 3) directly influence both mothers’ labor market participation and children’s development.
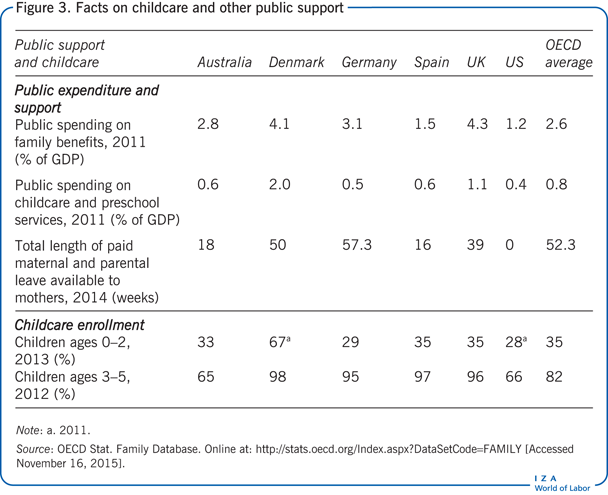
Parental leave policies, for example, have an impact on the timing of mothers’ labor market participation by guaranteeing a return to paid work after maternity leave and by minimizing the risk of dismissal during pregnancy. Almost all Western countries (with the notable exception of the US) offer a minimum period of 14 weeks’ maternity leave, as recommended by the International Labour Organization. In most OECD countries, parents are eligible for additional parental leave after maternity leave. This leave also protects parental employment, although pay may be lower during this period, unlike with maternity leave. The total length of maternity and parental leave available to mothers is presented in Figure 3. The OECD average combined leave is 52 weeks, although this rarely means 52 weeks at full pay. For example, parental leave is unpaid in the US, whereas in Denmark and Germany parental leave is partially paid and longer than elsewhere.
When parents are absent during the day, young children must spend that time elsewhere. Therefore, the relationship between maternal employment and childhood obesity depends greatly on where and how children spend this time. Research has shown that children benefit from high-quality childcare [5]. Thus, appropriate childcare is of great policy relevance. And independent of the type of childcare (informal or formal, private or public), both the availability and affordability of good quality childcare are important to parents.
Public spending determines the availability of high-quality and affordable formal childcare and preschool services. Public investment in childcare varies considerably across OECD countries, from 0.4% of GDP in the US to 2% of GDP in Denmark, which is far above the OECD average of 0.8% (see Figure 3). A comparison between the US and Denmark is especially revealing as empirical studies find ample evidence of a relationship between maternal employment and childhood obesity in North America but not in Denmark. Not surprisingly, Denmark also has the highest childcare enrollment rates for young children, at 67% for children ages 0–2 years and 98% for children ages 3–5 years. In other countries, low childcare enrollment rates coincide with low employment rates for mothers of children younger than 2 (Figure 2). The high child enrollment and mothers’ employment rates in Denmark suggest a relationship between the availability of high-quality childcare services, child enrollment rates, and mothers’ employment rates.
The affordability of high-quality childcare is also decisive for parents’ labor market decisions. Costs for childcare can be lowered through tax reductions for childcare spending, cash benefits, or subsidized childcare, which would also increase the returns to paid employment by reducing the share of wages that goes to childcare expenses. Public spending on family benefits is far above the OECD average (2.6% of GDP) in the UK (4.3%) and Denmark (4.1%). Enrollment rates in childcare are also high in both countries.
Timing and type of maternal work
The effects of maternal employment on childhood obesity also depend on how old the child is when the mother is employed. For example, research suggests that maternal full-time employment has its strongest effect on childhood obesity in mid-childhood (ages 5–10) [6]. One explanation could be that during this period children’s self-esteem, competence, and individuality undergo rapid changes. In particular, at a time when children are developing greater autonomy and facing higher expectations, their ability to think abstractly and apply new knowledge is still limited.
A mother’s longer working hours also appear to increase the risk of children being overweight or obese, especially in the case of highly educated mothers. One explanation is the implied time constraint: highly educated mothers work more hours on average and are more likely than less educated mothers to spend their time at home on health-promoting activities [7]. A child’s weight is also likely to be affected by the type of maternal employment, with negative health outcomes associated especially with non-standard work hours, long shifts, and long commutes.
There is also some evidence that the type and amount of maternal employment affects children’s health through different mechanisms [8]. First, a mother’s non-standard working hours (such as shift work) have a negative influence on children’s sleep. There is empirical evidence that children in families with mothers who work non-standard hours get around 1–1.5 fewer hours of sleep per week than children whose mothers stay at home, perhaps because mothers are not at home to supervise bed and wake times. Sleep is strongly related to obesity, so less sleep or lower quality sleep could increase childhood obesity. Second, mothers who work long hours (work intensity) may have less time and energy to spend with their children; they may also suffer from more stress and fatigue. Time-use research demonstrates that working mothers sleep less than non-working mothers. For both of these reasons, long or non-standard maternal working hours could directly influence childhood obesity [9].
A behind-the-scenes mechanism: Money versus time
The economics literature assumes that increased labor market participation of mothers leads to less time spent with their children. Thus, a trade-off exists between income and time: an increase in maternal income often comes at the expense of time to spend with children. Child health is influenced by genetic endowment, environmental factors, consumption of health-enhancing goods and services, and maternal and paternal time inputs. Parents influence their children’s health through investments in time and purchases of health-enhancing goods and services. For example, whereas money can pay for high-quality food, childcare, and extracurricular activities, time directly spent with children allows for the preparation of healthy meals, the provision of adequate supervision, and the monitoring of children’s engagement in physical activity.
Maternal employment and time spent with children
In economic terms, the 24 hours in each day can be distributed in various proportions among labor supply, household production, and leisure (including sleep). Clearly, if labor market supply increases, less time can be invested in other activities. Thus, the question is whether indeed less time is spent with children and on activities related to children’s diet and physical activity. Thereby, both the quantity of time invested and its quality matter.
Although working mothers generally spend less time with their children than do non-working mothers, time-use research shows that the differences are small [10]. If working mothers keep the time spent with their children at a fairly steady level, the implication is that they must spend less time on other activities, such as housework, leisure activities, volunteer activities, or sleep. One area of time savings is household production, where efficiency gains (because of smaller family size, household technical advances, convenience foods, and so on) have freed time to spend with children. However, mothers still do more child-related work at home than men, regardless of their work situation. Therefore, even though paternal time with children has increased in recent decades, fathers’ extra time with their children has not made up for all of the reduction in the time that working mothers spend with their children compared with non-working mothers [10].
When the total time that parents spend with children and on child-related activities is reduced, the quality of time together matters even more. For instance, research confirms that warm, loving, and consistent interactions between parents and children are most beneficial to child health outcomes [11]. Maternal employment can affect the quality of time spent with children in two opposite ways. If working mothers feel stressed by trying to maintain a work–family balance, maternal employment can have a negative effect on children’s health. However, if the financial and social benefits from work reduce parental stress, children may benefit. The quality of time spent with and for children is unfortunately often not observable and so is not directly measurable.
Also, mothers’ allocation of time for overseeing their children’s diet and physical activity potentially explains an association between maternal employment and childhood obesity. There is some evidence that working mothers spend less time than non-working mothers on diet-related activities such as grocery shopping and cooking [10]. The number of shared family meals may also decline. Studies find that family meals benefit children’s health and that children who spend less time eating with the family have less nutritious and higher fat diets [9]. The relevant question is thus where children eat and what they eat when they do not eat at home. Although there is no consensus on how much a mother’s work affects the diet quality of her children, some studies point to a decrease in children’s intake of fruits and vegetables [9], while others do not find such a reduction [1]. Children of working mothers eat more meals outside the home. Out-of-home meals are generally linked to a higher risk of childhood obesity because they are often high in fat, sugar, and salt and have a lower nutrient density than foods prepared at home.
In addition, children’s level of physical activity might be reduced if mothers spend less active time with their children. Children could then choose more of their activities by themselves (studies find more sedentary behavior when children choose their own activities) or spend more time in childcare, where the level of activity depends on the quality of the childcare provider. Only a few studies discuss the relation between maternal employment and child dietary behavior and physical activity, and those that do draw inconsistent conclusions. For example, whereas some studies conclude that sedentary behavior such as watching television increases when highly educated mothers work [9], other studies find no such relation, implying that maternal employment has no effect on a child’s physical activity [1].
Maternal employment and higher income
When mothers work more, household income goes up. There is ample evidence of a strong relation between a family’s socio-economic status and obesity in children: children who grow up in poverty are more likely to be overweight or obese than children who grow up in wealthier households. Thus, if maternal employment helps a family escape poverty, it could be beneficial to children’s weight outcomes. A higher household income could also benefit children’s health by enabling families to purchase goods and services that can substitute for mothers’ time engaged in household production, such as cleaning and other domestic services. It can also enable families to buy better quality food, sign up children for organized sports activities or athletic club memberships, or pay for higher quality childcare. The counter argument is that higher income will not necessarily be invested in higher quality foods or childcare. However, it is also possible that mothers with higher labor market skills (and thus with higher incomes) may be more likely to invest in their children’s health.
Limitations and gaps
Whether maternal employment increases the likelihood of a child becoming overweight or obese is a straightforward question. Answering that question, however, involves major methodological challenges, including difficulties in measuring childhood obesity, a lack of data, and concerns about reverse causality. Not only do few countries have adequate systems for monitoring childhood overweight and obesity rates, but data, if available at all, tend to be reported infrequently and are often based on self-reported measures of body mass index. Another data-related problem is the inability to determine whether maternal employment affects childhood obesity or whether childhood obesity affects maternal employment (for example, if a mother decides to stay home because her child is obese). The longitudinal data needed to control for reverse causality are scarce and thus form the basis of only a few studies.
It is important to better understand the still largely underexplored mechanisms behind the potential relationship between maternal employment and childhood obesity. Both the mother’s employment status and the child’s health status could be influenced by unobservable maternal characteristics, such as high ability. If that is true, maternal employment would not necessarily be an explanatory factor in childhood obesity but could be spuriously correlated with it. High ability of mothers, for example, could be the original factor driving both mothers’ working more hours and caring better for their children’s health [1]. In economics, this is called endogeneity. If mothers’ ability is the underlying driving factor, the relationship between maternal employment and childhood obesity would be underestimated. On the other hand, mothers who work more could be less attentive to their children’s health, which would lead to overestimation of the effect of maternal employment on childhood obesity. The potential bias could also differ by country or context. For instance, in Scandinavian countries, most mothers are employed full-time, so women who work fewer hours are a deviation from the norm [1]. Working fewer hours could indicate lower ability, which would suggest worse outcomes for child health. Possible solutions for such endogeneity problems would be the use of rich information on child and family characteristics or an instrumental variable approach (a statistical technique used when omitted variable bias, measurement error, or reverse causality are suspected), both of which have their own methodological drawbacks.
Summary and policy advice
The governing research question for this discussion is whether maternal employment affects childhood obesity. According to a wide body of research conducted in the US, maternal employment is associated with higher rates of childhood obesity, supporting the argument made by some people that mothers should stay at home. However, it is not that simple. If mothers stay at home, household income is lower, and there is clear evidence that children in lower-income households, especially in households below the poverty line, are more likely to be overweight or obese. Thus, encouraging mothers not to work will not necessarily translate into better child health. Actually, empowering families with dual incomes could help to fight obesity.
Studies for Denmark shed some light on the mechanisms through which maternal employment could have beneficial effects on child health. The beneficial effects of maternal employment on childhood obesity observed in Denmark may be a result of the high-quality formal childcare provided in that country. If high-quality childcare means that children have access to nutritious diets and physical activity outside their home and if this childcare is available to all working families, then it should not matter for child development whether mothers work or not. Intuitively, it seems logical that high-quality childcare, whether provided by the family (mother, father, and extended family) or by formal institutions and some informal care, would enhance child development. Policy measures should thus aim at providing working parents with greater flexibility to spend more time with their children (by promoting parental leave, for example) and at developing high-quality and affordable formal childcare.
Parents’ influence on children is often limited by the environment in which the family lives, including the physical, media, social, commercial, and educational environment. For example, poor urban neighborhoods have higher than average fast-food restaurant density, fewer grocery stores (food deserts), and low walkability, promoting unhealthy diets and sedentary behavior. Instead of debating whether mothers should work, policies should aim at enhancing “junk food free” environments.
Acknowledgments
The author thanks two anonymous referees and the IZA World of Labor editors for many helpful suggestions on earlier drafts. The author’s previous work contains a larger number of background references for the material presented here and has been used intensively in all major parts of this article [1]. Feedback from Alfonso Sousa-Poza and Peng Nie is gratefully acknowledged.
Competing interests
The IZA World of Labor project is committed to the IZA Guiding Principles of Research Integrity. The author declares to have observed these principles.
© Wencke Gwozdz
Measuring childhood obesity
Often, what is actually measured is not obesity but whether a child is overweight (excess weight in relation to height), which can be measured by the body mass index (BMI). BMI—calculated as weight (kg)/height2 (m2)—is the most used indicator of being overweight because it is inexpensive and easy to measure.
However, BMI is problematic, particularly in children, in that it varies strongly according to sex and age. As a result, the significance of any particular BMI is more difficult to determine in children and adolescents. BMI also measures fat-free weight, meaning that individuals with the same BMI can have different amounts of body fat. Moreover, self-reports of height and weight are systematically biased—especially when reported by parents—leading to over- and under-estimation of BMI, especially at the end points (being thin or overweight; Himes, 2009).In adults, the BMI cut-off points for when being overweight becomes detrimental are associated with a morbidity risk that is well established. This information is lacking for children. For that reason, growth charts are used when defining a benchmark BMI distribution according to sex and age. This benchmark population was established in the “pre-obesity epidemic” era and remains in use today as a reference population. A growth chart is a visual presentation of a growth reference. Individuals can be plotted on the chart and their measurements expressed as centiles indicating a child’s BMI by age and sex. The growth references determine whether a child is obese, overweight, or normal weight. For example, a child who crosses the 95th centile line for their age and sex would be categorized as obese. Well-known examples of growth charts are the Center for Disease Control growth charts for the US and the International Obesity Task Force growth charts based on six countries and used in international contexts.Source: Himes, J. H. “Challenges of accurately measuring and using BMI and other indicators of obesity in children.” Pediatrics 124:S1 (2009): S3–S22; Sweeting, H. N. “Measurement and definitions of obesity in childhood and adolescence: A field guide for the uninitiated.” Nutrition Journal 6:1 (2007): 32.